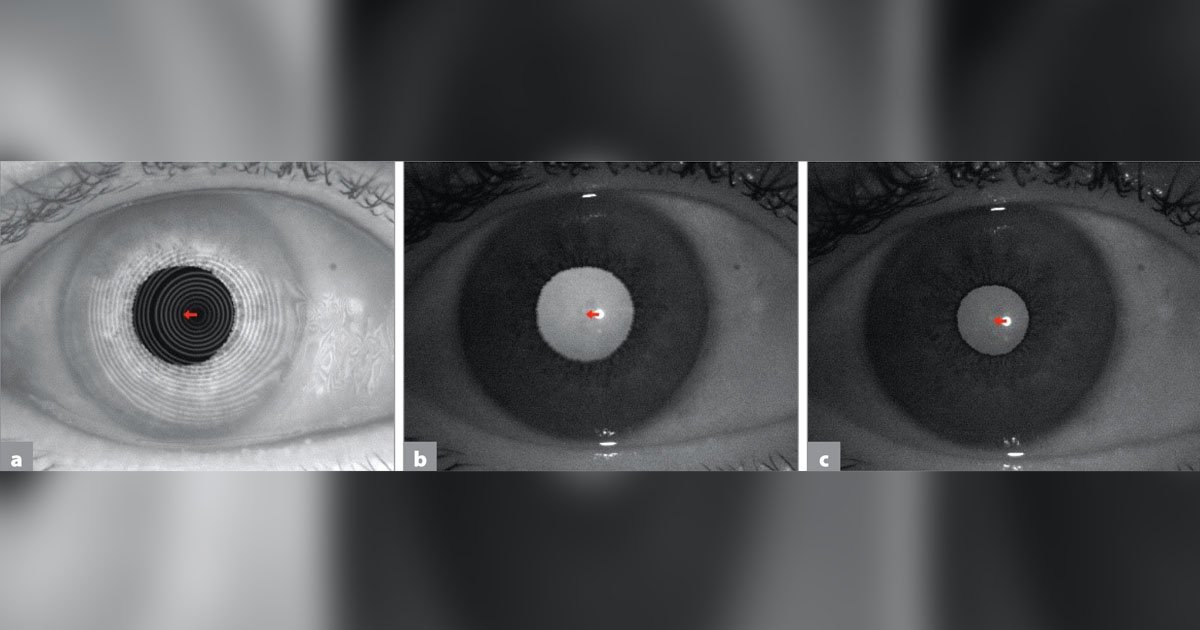
Atlas 9000 images of the same eye. In this patient, chord mu changes only slightly under different lighting conditions. Rings image (a). Scotopic pupil image (b). Photopic pupil image (c).
IOLs must be centered precisely to achieve optimal refractive outcomes from advanced lens technology.
To assist with centration, clinicians have used ocular angles, such as angle kappa, to describe the gap between the visual axis and the pupillary axis. However, there have been conflicting definitions when using these terms.
Historically, various terms have been used to describe reference axes. The visual axis represents the line from the fixation point through the nodal point, with the assumption that this line connects with the fovea. However, this is only a theoretical construct. In reality, no ray of light connects the fixation point to the fovea in a straight line because it bends at four refractive interfaces. Furthermore, with no visible reference point, the theoretical concept of the visual axis does not help a surgeon center an IOL. Nevertheless, the term visual axis remains a popular way to describe the axis on which surgeons like to align treatments. The pupil does not typically align on this axis, frequently lying slightly nasally or superiorly. Therefore, we have a discrepancy between the center of the pupil (a reference point for both the pupillary axis and line of sight) and the so-called visual axis.
Because of these discrepancies and inconsistencies, Dr. George Waring IV and I introduced the concept of the subject-fixated coaxially sighted corneal light reflex (SF-CSCLR) as a reproducible clinical marker for IOL centration. As the patient fixates on a light source, light reflects from the cornea. The corneal light reflex is viewed or captured coaxially and provides a reproducible reference point — the SF-CSCLR for centration. While not technically equivalent, the terms visual axis and corneal vertex have traditionally been used synonymously with the location defined by the SF-CSCLR and the line connecting the SF-CSCLR to the fixation point (the SF-CSCLR axis). A number of devices, such as the IOLMaster, Atlas corneal topography system, and Lumera operating microscope (all Zeiss), can be used to locate the SF-CSCLR. Because the light reflex is not affected by pupil dilation, it is a reproducible marker that carries through preoperatively, intraoperatively and postoperatively. This is where I align IOLs.
Because the measurement between the SF-CSCLR axis and the pupil center is a chord distance and not an angle, we introduced the concept of chord mu or the CW-chord (Chang-Waring chord). Chord mu or CW-chord is the more accurate term; nevertheless, for centration purposes, many surgeons still commonly use it interchangeably with the term angle kappa.
Integration into technology
To help surgeons apply this clinically, we have been working with manufacturers that have integrated these measures into a range of devices. Although some technologies use x and y Cartesian coordinates to express chord mu, others now describe chord mu or the CW-chord in our preferred radial notation as millimeters at an angle.
While many diagnostic devices measure the distance from the visual axis to the pupil center, there is a lack of consistency on how the information is reported. The IOLMaster 700 presents this displacement as the CW-chord or chord mu (Figure 1), and the Atlas 9000 presents the same quantity in Cartesian (x-y) coordinates (Figure 2). Different devices measure the quantitative separation of the visual axis and the pupil center with varying techniques and present it as different quantities. It is important to know what your particular device is actually measuring and how that relates to what you are trying to achieve.
Application of measurements
When examining patients preoperatively, I do not look for a specific chord mu to exclude a patient as a potential candidate for a presbyopic IOL. Instead, I examine the eye image, looking for a pupil that is round and fairly centered. If a patient has obvious pupil abnormalities or gross corectopia, perhaps greater than 0.8 mm, I would consider avoiding a diffractive presbyopia-correcting IOL.
While decentration can negate the benefits of asphericity and increase dysphotopsias, a large preoperative chord mu does not necessarily predict postoperative IOL decentration. This is because the IOL performs ideally when centered on the visual axis as represented by the SF-CSCLR and not on the pupil. While it is easier to see whether an IOL lines up with the pupil center, the IOL should actually be lined up with the visual axis. In other words, while a large preoperative chord mu may result in an IOL decentered from the pupil center, it does not mean that the IOL is decentered from the visual axis.
Intraoperative steps
When I am centering an IOL during surgery, it does not matter where the pupil center lies or what chord mu is because both change with dilation. Therefore, I do not worry about the pupil location; my target is the SF-CSCLR. In particular, I center an IOL on the light reflex of a microscope that has true coaxial illumination, such as the Lumera. After switching off the oblique light, I have the patient fixate on one of the two stereo coaxial lights. Because each coaxial light lines up with one of my oculars, I have the patient fixate on the light that corresponds to the ocular that I use for viewing that step. Because my microscope camera is on the left ocular, I have the patient fixate on the left light, and I use my left eye to sight it.
For additional guidance, the Callisto eye (Zeiss) alignment device can determine the same fixated CSCLR point based on preoperative measurements from the IOLMaster 700.
The nice thing about this approach is that when performing surgery, I do not have to be concerned about preoperative ocular axes and angles; rather, I simply focus on intraoperative light reflexes and center my IOLs accordingly.
It is important to realize that different lenses vary in their tolerance to decentration. If a lens is decentered from the visual axis, the result will primarily be induced astigmatism. Therefore, if the IOL is off-center from the visual axis, a refractive correction such as a laser enhancement can be performed to optimize the visual outcome.
Conclusion
Precise IOL centration is necessary to achieve optimal visual outcomes from cataract surgery. However, inconsistencies persist in the description of ocular reference axes and quantifying the distance between axes. Reproducible reference points such as those discussed in this article are necessary to achieve IOL centration and predictable results with advanced technology IOLs.
more recommended stories
 Texas Medical Board Releases Abortion Training for Physicians
Texas Medical Board Releases Abortion Training for PhysiciansKey Takeaways Texas Medical Board has.
 Safer Allogeneic Stem Cell Transplants with Treg Therapy
Safer Allogeneic Stem Cell Transplants with Treg TherapyA new preclinical study from the.
 Autoimmune Disorders: ADA2 as a Therapeutic Target
Autoimmune Disorders: ADA2 as a Therapeutic TargetAdenosine deaminase 2 (ADA2) has emerged.
 Kaempferol: A Breakthrough in Allergy Management
Kaempferol: A Breakthrough in Allergy ManagementKaempferol, a dietary flavonoid found in.
 Early Milk Cereal Drinks May Spur Infant Weight Gain
Early Milk Cereal Drinks May Spur Infant Weight GainNew research published in Acta Paediatrica.
 TaVNS: A Breakthrough for Chronic Insomnia Treatment
TaVNS: A Breakthrough for Chronic Insomnia TreatmentA recent study conducted by the.
 First-of-Its-Kind Gene-Edited Pig Kidney: Towana’s New Life
First-of-Its-Kind Gene-Edited Pig Kidney: Towana’s New LifeSurgeons at NYU Langone Health have.
 Just-in-Time Training Improves Success & Patient Safety
Just-in-Time Training Improves Success & Patient SafetyA study published in The BMJ.
 ChatGPT Excels in Medical Summaries, Lacks Field-Specific Relevance
ChatGPT Excels in Medical Summaries, Lacks Field-Specific RelevanceIn a recent study published in.
 Study finds automated decision minimizes high-risk medicine combinations in ICU patients
Study finds automated decision minimizes high-risk medicine combinations in ICU patientsA multicenter study coordinated by Amsterdam.
Leave a Comment